Page Contents
Infection Prevention and Control (IPC) has become one of the most important pillars of nursing home operations. The COVID-19 pandemic demonstrated how rapidly infectious diseases can spread within residential care settings and how devastating the consequences can be for vulnerable older adults.
While healthcare advances have significantly improved longevity, infectious diseases continue to pose a major threat to elderly populations due to age-related decline in immunity, multiple chronic illnesses, and communal living environments. Strengthening IPC measures is therefore not only a regulatory requirement but a critical responsibility in safeguarding residents’ health, dignity, and quality of life.
What are infectious diseases?
Infectious diseases are illnesses caused by microorganisms such as bacteria, viruses, fungi, or parasites that invade the body and multiply. These organisms can spread from person to person, through contaminated surfaces, through the air, or via contact with bodily fluids.
In nursing homes, infectious diseases can spread rapidly because residents live in close proximity, share common spaces, and often require assistance with activities of daily living. Many elderly residents also have weakened immune systems, making them more susceptible to infections and their complications.
Examples of infectious diseases include influenza, COVID-19, pneumonia, tuberculosis, norovirus, urinary tract infections, and skin infections.
Infectious disease rates in eldercare facilities
Infectious diseases remain one of the leading causes of hospitalisation and mortality among nursing home residents worldwide.
Studies estimate that between 1 and 3 million serious infections occur annually in long-term care facilities globally. At any given time, approximately 1% to 5% of nursing home residents may have an active healthcare-associated infection.
Respiratory infections are among the most common outbreaks in eldercare facilities. Influenza, COVID-19, respiratory syncytial virus (RSV), and pneumonia continue to account for substantial morbidity and mortality among older adults.
Research has also shown that a single outbreak within a nursing home can affect a large proportion of residents within days if appropriate infection control measures are not implemented promptly.
These statistics highlight the importance of maintaining a robust IPC programme even when there are no active outbreaks.
Common infectious diseases in nursing homes
Several infectious diseases are frequently encountered in eldercare settings.
Respiratory Infections
Respiratory infections spread easily in communal environments and often result in outbreaks.
Common examples include:
- COVID-19
- Influenza
- Respiratory Syncytial Virus (RSV)
- Pneumonia
- Tuberculosis
Gastrointestinal Infections
These infections can spread rapidly through contaminated food, water, hands, or surfaces.
Common examples include:
- Norovirus
- Rotavirus
- Foodborne illnesses
Urinary Tract Infections (UTIs)
UTIs are particularly common among residents with urinary incontinence, indwelling catheters, diabetes, or reduced mobility.
Skin and Soft Tissue Infections
Skin infections may occur due to wounds, pressure injuries, fungal infections, or poor skin integrity.
Common examples include:
- Cellulitis
- Scabies
- Fungal infections
- Infected pressure ulcers
Multidrug-Resistant Organisms (MDROs)
Healthcare settings increasingly encounter resistant organisms such as:
- MRSA (Methicillin-resistant Staphylococcus aureus)
- VRE (Vancomycin-resistant Enterococcus)
- ESBL-producing bacteria
- Carbapenem-resistant organisms
How serious are these diseases for the elderly?
Infections affect older adults differently from younger individuals. As people age, their immune systems become less effective at fighting infections. Chronic illnesses such as diabetes, heart disease, kidney disease, dementia, and chronic lung disease further increase vulnerability.

In some cases, elderly residents may not develop typical symptoms such as fever. Instead, infections may present as confusion, reduced appetite, weakness, falls, or sudden behavioural changes, making early detection more challenging. A seemingly minor infection can therefore rapidly progress into a life-threatening condition.
Chain of Infection
The Chain of Infection is a fundamental concept in infection prevention and control. Infection occurs when all six links of the chain are connected.
- Infectious Agents – bacteria, virus, fungus, or parasite
- Reservoir – where the organism lives and multiplies
- Portal of Exit – how the organism leaves the source
- Mode of Transmission – how it spreads
- Portal of Entry – how it enters a new host
- Susceptible Host – a person vulnerable to infection
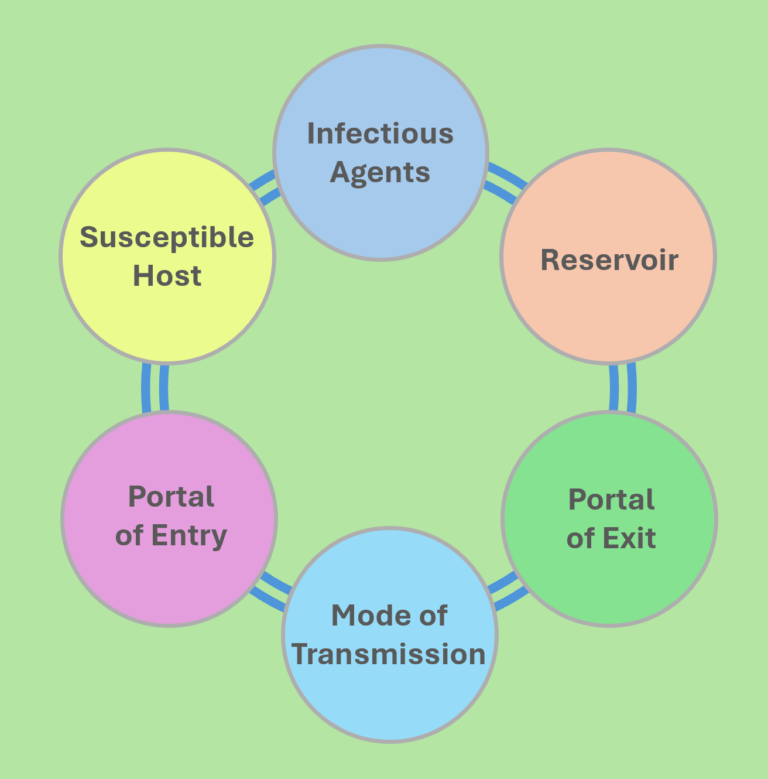
The key principle of IPC is to break one or more links in this chain. Examples include:
- Hand hygiene interrupts transmission.
- Environmental cleaning removes reservoirs.
- Masks reduce portals of exit and entry.
- Vaccination reduces host susceptibility.
- Isolation prevents transmission to others.
Every IPC measure implemented in a nursing home ultimately aims to break the chain of infection.
Strategies and considerations for disinfection
Effective disinfection goes beyond simply spraying disinfectant. Several factors determine whether disinfection is successful:
Appropriate product selection
Different microorganisms require different disinfectants. Facilities should ensure products are approved, effective, and used according to manufacturer instructions.
Cleaning before disinfection
Organic matter such as dirt, food residue, blood, and body fluids can reduce disinfectant effectiveness. Cleaning should always precede disinfection when surfaces are visibly soiled.
Contact time
Many disinfectants require surfaces to remain wet for a specific duration to achieve microbial kill. Wiping surfaces dry too quickly reduces effectiveness.
High-touch surface focus
Priority should be given to frequently touched surfaces such as:
- Bed rails
- Door handles
- Lift buttons
- Handrails
- Wheelchairs
- Dining tables
- Call bells
Staff competency
Even the best disinfectant will fail if staff are not properly trained. Regular audits and competency assessments are essential.
When not to do misting?
Not all infectious diseases can be effectively controlled through misting or fogging. The choice of disinfection method should always be based on how the disease spreads.
- Airborne diseases (e.g., tuberculosis) are best controlled through proper ventilation, air filtration, and respiratory protection. Misting does not remove infectious particles suspended in the air.
- Contact-transmitted diseases (e.g., norovirus and MDROs) require thorough cleaning and direct disinfection of frequently touched surfaces. Manual wiping is often more effective than misting alone.
Scabies is a good example where misting is generally not effective. Scabies mites spread mainly through direct skin contact and contaminated clothing, bedding, and linens. Control measures should focus on treatment of affected individuals, laundering of fabrics, environmental cleaning, and isolation precautions.

Misting may serve as a supplementary disinfection tool in selected situations, but it should never replace fundamental IPC practices such as hand hygiene, environmental cleaning, staff education, and transmission-based precautions.
Conclusion
Infectious diseases will always remain a challenge in nursing homes due to the vulnerability of elderly residents and the communal nature of long-term care environments. However, outbreaks are not inevitable.
A strong Infection Prevention and Control programme built upon surveillance, staff training, hand hygiene, environmental cleaning, vaccination, and prompt outbreak management can significantly reduce infection risks.
The lessons learned from recent global outbreaks have reinforced a simple but powerful message: Prevention is Better Than Cure. Every infection prevented means one less hospitalisation, one less complication, and one more opportunity for an elderly resident to enjoy a safer, healthier, and more dignified life.
Caring for our ageing loved ones is a journey filled with questions, challenges, and important decisions. If you are supporting an elderly parent or caring for someone with memory loss, my ebooks, When They Need You: A Family Guide to Caring for Aging Parents and When the Mind Fades: A Family Guide to Dementia and Cognitive Decline, provide practical guidance, compassionate insights, and real-world advice for families and caregivers.
To learn more about these books and explore additional resources on ageing and eldercare, click the link Here to visit my ebook page. You do not have to navigate the ageing journey alone.